Mastering clinical documentation is a cornerstone of effective mental health practice. For counselors, therapists, and social workers, utilizing a structured format ensures clarity, continuity of care, and compliance with ethical and legal standards. This is why understanding and implementing a robust Soap Notes Counseling Template is essential for streamlining administrative tasks while maintaining high-quality patient records. These notes serve as the primary communication tool among providers, supporting treatment planning, justifying billing, and providing a historical record of therapeutic interventions.
The adoption of the SOAP format transcends mere clerical duty; it is an active component of clinical reasoning. By forcing the practitioner to categorize observations, assessments, and plans systematically, the template promotes focused reflection on the client’s progress. In today’s complex healthcare environment, where interdisciplinary collaboration is common, a standardized yet adaptable documentation structure like SOAP ensures that critical information is accessible, concise, and actionable for anyone reviewing the client’s file.
Many practitioners struggle to balance thorough documentation with the time constraints of a busy schedule. A well-designed template minimizes this friction, providing guardrails that guide the clinician through necessary data points without stifling the nuance of the therapeutic encounter. Whether you are a seasoned professional or just beginning your journey in private practice or agency work, optimizing your approach to case notes directly impacts both efficiency and the caliber of care delivered.
This comprehensive guide will dissect the components of an ideal Soap Notes Counseling Template, explore best practices for its completion, and discuss how digital tools can enhance this vital record-keeping process, ultimately solidifying your professional standing and improving client outcomes.
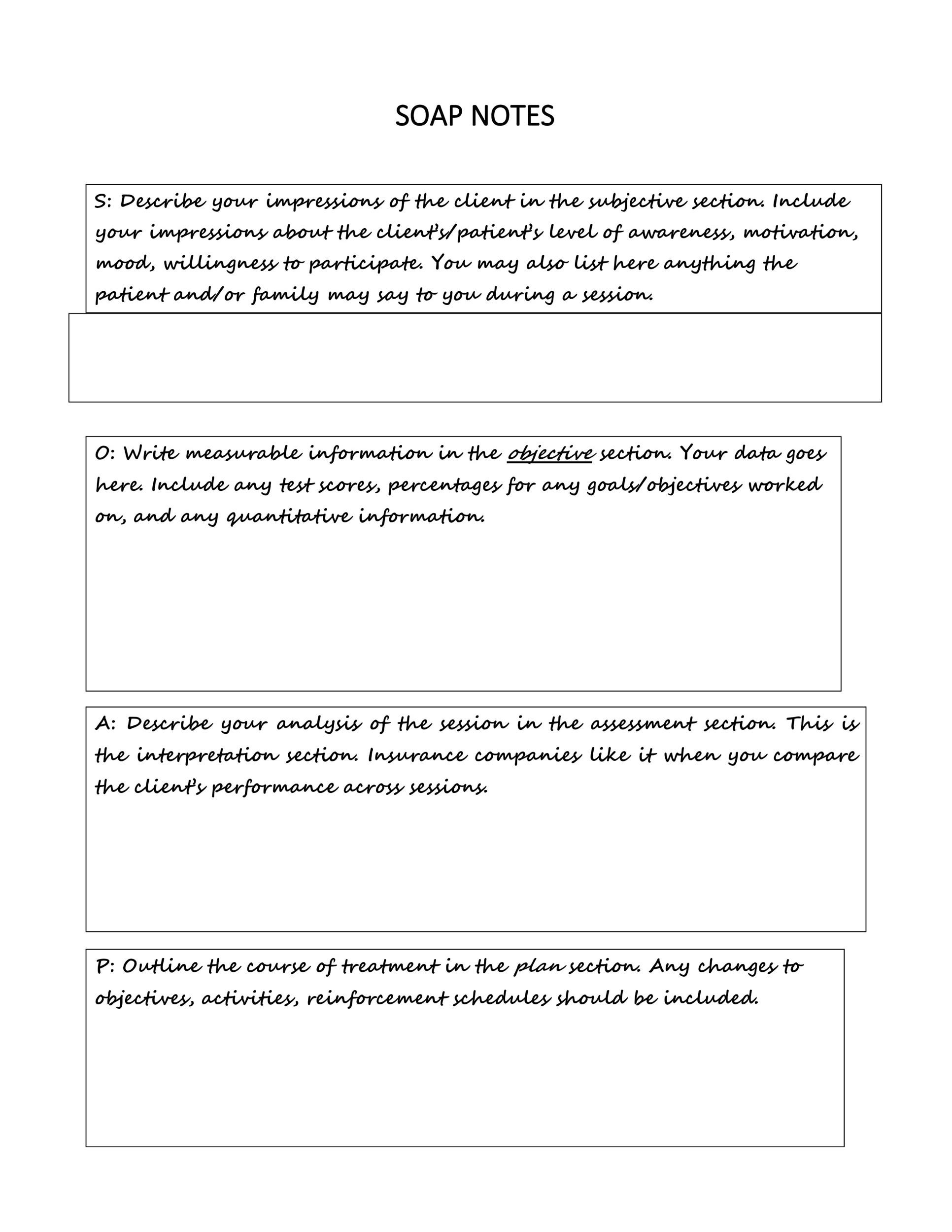
The SOAP methodology, originating in medical charting, stands for Subjective, Objective, Assessment, and Plan. While its roots are clinical, its structure translates perfectly to the nuances of counseling and psychotherapy, providing a flexible yet rigorous framework for capturing the essence of each session.

The Subjective section is where you document what the client says and how they present themselves, using their own words whenever possible. This captures the client’s perspective, feelings, and reported experiences since the last session.

For counseling, the Subjective component often includes:
* Client’s chief complaint or reason for coming to the session.
* Reported mood and affect (e.g., “Client reported feeling overwhelmed by work stress,” or “Patient stated, ‘I haven’t slept well all week'”).
* Updates on stated goals or homework assigned in the previous session.
* Any significant life events or symptoms reported by the client.

Capturing the client’s narrative accurately is crucial for establishing rapport and ensuring treatment remains client-centered. Avoid interpretation here; stick to direct quotes or clear paraphrasing of the client’s self-report.

The Objective section details verifiable observations made by the counselor during the session. Unlike the Subjective section, this data should be measurable, observable, and factual, independent of the client’s interpretation.

Examples relevant to a counseling setting include:
* Appearance and Demeanor: Note hygiene, posture, eye contact, and grooming.
* Affect and Mood: Observable emotional expressions (e.g., “Affect was restricted, flat,” or “Tearful at moments when discussing family dynamics”).
* Speech Patterns: Rate, volume, and coherence (e.g., “Speech was pressured,” or “Speech was slow and monotone”).
* Engagement: Level of participation, collaboration, and insight demonstrated during the session.
* Mental Status Exam (MSE) findings that are externally visible, such as thought process coherence.
This section provides the concrete evidence that supports the subsequent assessment.
The Assessment is the synthesis of the Subjective and Objective information. This is where the counselor applies their Expertise to interpret the data gathered and determine the client’s current clinical status, progress, and diagnostic considerations.
A strong Assessment section should include:
* A summary statement regarding overall progress (e.g., “Client demonstrated slight improvement in distress tolerance compared to the last session.”).
* Analysis of symptoms and functional impairment relative to the diagnosis.
* Hypotheses regarding underlying dynamics or triggers observed.
* Identification of any immediate risks or barriers to progress.
This section demonstrates your clinical reasoning. It moves beyond simply reporting facts to explaining why the client is presenting as they are and how the interventions are theoretically aligning with their needs.
The Plan details the next steps for treatment, both within the immediate session context and moving forward. This element is vital for continuity and justifying the necessity of future appointments.
The Plan typically covers:
* Interventions used during the session (e.g., “Utilized 10 minutes of deep diaphragmatic breathing techniques to practice grounding.”).
* Homework assigned to the client for the coming week (e.g., “Client agreed to log three instances of challenging thoughts daily.”).
* Goals for the next session (e.g., “Next session will focus on challenging cognitive distortions related to perfectionism.”).
* Consultation or referral plans, if necessary.
A clear Plan shows the client (and any reviewer) that the session was goal-directed and purposeful.
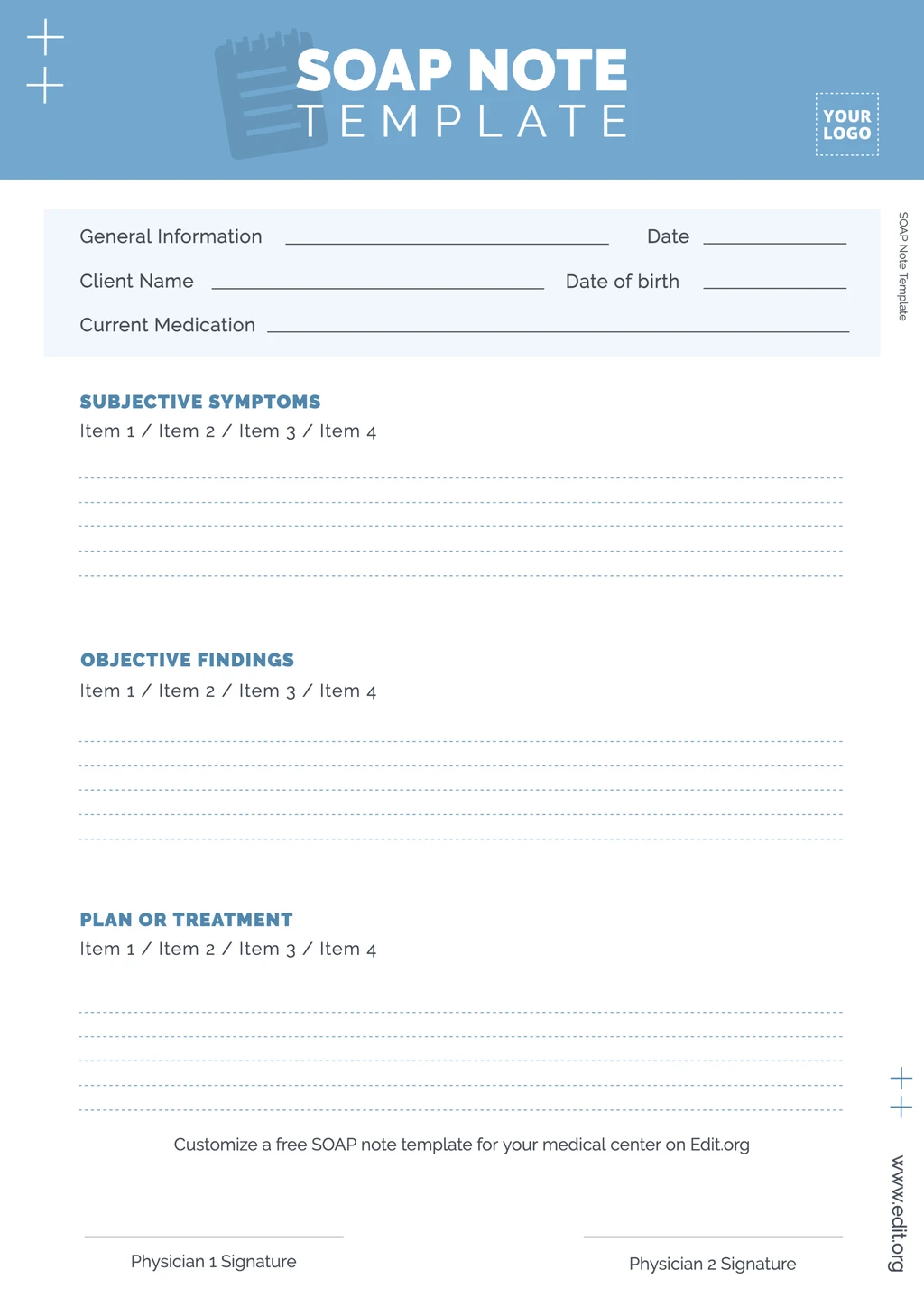
Creating a standardized Soap Notes Counseling Template requires balancing necessary structure with the flexibility to capture diverse clinical presentations. Customization based on your specialty (e.g., LPC, LMFT, LCSW) and preferred modality (e.g., CBT, DBT, Psychodynamic) is key to efficiency.
While the S-O-A-P structure is universal, the language within the O and A sections must reflect your theoretical orientation.
If you practice Cognitive Behavioral Therapy (CBT), your template prompts might include:
* O: Notation of automatic negative thoughts recorded or challenged.
* A: Assessment of core beliefs currently being reinforced or challenged.
* P: Plan to introduce a new thought record or behavioral experiment.
If your work leans toward Humanistic or Person-Centered Therapy, your template should prioritize:
* S: Detailed documentation of self-exploration and congruence experienced by the client.
* A: Counselor’s assessment of the therapeutic relationship’s quality and movement toward self-actualization.
To enhance objectivity (O) and streamline assessment (A), incorporating brief, standardized scales directly into your template can be highly beneficial. This adds measurable data points that demonstrate progress over time—a requirement for many insurance payers seeking evidence of treatment efficacy.
Consider embedding short self-report measures such as:
* A 1-10 rating of current distress level.
* A quick check-in on anxiety or depression symptoms using a simple scale (e.g., PHQ-2 or GAD-2 elements).
* Client rating of therapeutic alliance for that session.
These additions provide quantifiable data that anchors your subjective experience in measurable outcomes, significantly boosting the Authoritativeness of your records.
In the realm of mental health documentation, E-E-A-T—Experience, Expertise, Authoritativeness, and Trustworthiness—is paramount. Your SOAP notes are primary evidence of these qualities.
Your notes should reflect seasoned professional judgment. This means moving beyond simple description toward skilled interpretation. If you are documenting a complex trauma presentation, your Assessment section, informed by your Experience, should clearly connect the client’s subjective reports (S) to established trauma responses (A), justifying your choice of evidence-based intervention (P).
For instance, instead of just noting, “Client cried when talking about mother,” an expert note might read: “Client exhibited hyperarousal, characterized by rapid speech and shallow breathing (O), during discussion of early attachment figures. Assessment suggests activation of unresolved relational trauma schemata, necessitating grounding techniques before proceeding further next week (P).”
Trustworthiness hinges on accuracy and confidentiality. Always double-check that demographic information is correct and that your documentation strictly adheres to HIPAA regulations. Never include identifying information of other clients or extraneous personal details.
Furthermore, trustworthiness is built through consistency. Utilizing a consistent Soap Notes Counseling Template ensures that all critical components are addressed for every client, every time, making the record dependable for peer review or audits. If you are integrating data from external sources—such as psychiatric evaluations or collateral contacts—ensure these sources are clearly cited within the Objective or Assessment sections.
While paper notes offer simplicity, modern practice management software (PMS) and electronic health record (EHR) systems offer robust tools that enhance the functionality and security of your SOAP documentation.
Digital templates allow you to pre-load frequently used information, such as your standard treatment goals, evidence-based intervention descriptions, and specific diagnostic criteria codes (ICD-10). This drastically reduces typing time. A well-programmed system can auto-populate standard information, allowing the counselor to focus their energy on tailoring the S, A, and P sections to the unique needs of the session.
Trustworthiness in the digital age heavily relies on robust security. Cloud-based, encrypted EHR systems are designed to meet stringent regulatory requirements far exceeding the security of a locked filing cabinet. They also offer powerful search capabilities. A clinician can quickly pull up all notes referencing a specific symptom (e.g., “insomnia”) across multiple months, providing a longitudinal view that is crucial for tracking treatment effectiveness.
Advanced EHR systems link the SOAP note directly to outcome tracking. If you utilized a standardized depression inventory in the Objective section this week, the system can automatically chart that score against previous weeks, providing immediate visual feedback in the Assessment section regarding patient trajectory. This data-driven approach strengthens the Authoritativeness of your clinical decisions.
Even with a clear template, practitioners frequently fall into common documentation traps that diminish the quality and defensibility of their notes. Recognizing these pitfalls is crucial for elevating your record-keeping.
A note that consists almost entirely of copied or summarized client statements (heavy on ‘S’ and light on ‘A’ and ‘P’) is insufficient. If the Assessment section is thin, it suggests the counselor failed to integrate the subjective report with clinical knowledge. The client’s report sets the stage, but the professional assessment must interpret the scene.
One of the most frequent errors is placing clinical interpretations within the Subjective section. For example, writing in ‘S’: “Client seems depressed.” This is an interpretation. The Subjective section should be “Client stated, ‘I feel hopeless today.'” The Assessment section is where you record: “Client appears depressed based on slowed psychomotor activity and constricted affect.” Maintaining this strict delineation upholds the integrity of the Soap Notes Counseling Template.
A weak Plan section often leads to disorganized follow-up. If the Plan simply says, “Continue treatment,” it fails to document a defensible rationale for the next billable session. Every note must justify the need for the next appointment. If the Plan is vague, the entire session documentation lacks clinical direction.
In many billing scenarios, the duration of the session is a critical component. Ensure your template includes fields for the start and end time of the service, and the total time spent providing direct client contact. Lack of precise timing can complicate billing compliance and accountability.
While SOAP notes are standard for routine sessions, their structure is equally valuable, if not more so, during high-risk or crisis interventions. In these scenarios, speed, clarity, and thoroughness are non-negotiable.
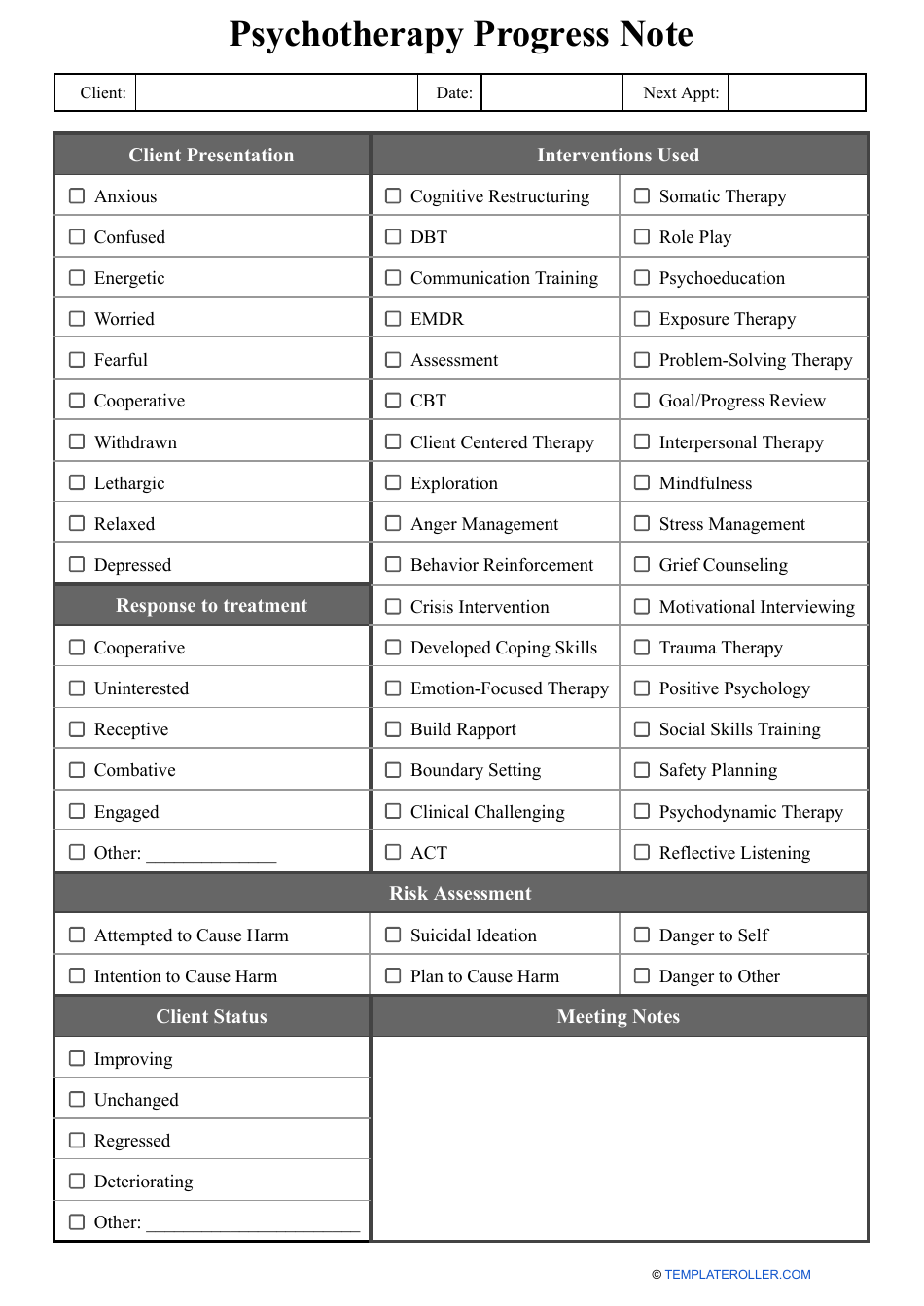
The Subjective section must clearly capture the severity of the expressed crisis: suicidal ideation (SI), homicidal ideation (HI), recent attempts, intent, plan, and access to means. Direct quotes regarding intent are invaluable here.
The Objective section needs to document observable risk factors meticulously: client’s affect (e.g., highly agitated, flat/numb), level of cooperation with safety planning, motor activity, and presence of any intoxication or withdrawal signs.
The Assessment must synthesize these factors into a clear risk level determination (e.g., “Low risk due to good protective factors and willingness to contract for safety,” or “High risk requiring immediate hospitalization due to specific plan and lack of protective factors”). This judgment is the core demonstration of your clinical Expertise.
The Plan must be concrete and immediate: who was contacted (e.g., emergency contact, crisis team), what safety agreements were established, and if the client was transported to an emergency facility. The plan needs to be executable and auditable.
The Soap Notes Counseling Template is far more than a bureaucratic hurdle; it is the scaffolding upon which strong, ethical, and clinically effective mental health care is built. By rigorously applying the Subjective, Objective, Assessment, and Plan framework, practitioners ensure comprehensive capture of the therapeutic encounter, demonstrating clinical reasoning rooted in Experience and Expertise. Proper implementation—paying close attention to objective evidence, synthesizing data in the assessment, and detailing actionable plans—solidifies the Authoritativeness and Trustworthiness of the professional record. In the evolving landscape of healthcare, mastering this foundational documentation technique remains indispensable for optimizing workflow, meeting compliance demands, and, most importantly, providing the highest standard of client care.