Mastering documentation is a cornerstone of effective clinical practice, and utilizing a robust Psychology Progress Note Template is essential for maintaining clinical rigor, ensuring continuity of care, and meeting legal and ethical standards. These templates serve as the backbone of a therapist’s record-keeping, transforming complex session interactions into structured, auditable data points. They are not merely bureaucratic hurdles; rather, they are powerful tools that facilitate clinical reflection, demonstrate medical necessity, and streamline billing processes. For any mental health professional, from an intern to a seasoned practitioner, standardizing documentation through a well-designed template significantly reduces cognitive load during charting, allowing more focus to remain on client well-being.
The demands placed upon mental health clinicians today require efficiency without sacrificing detail. In an era of increased scrutiny from insurance providers, regulatory boards, and ethical committees, the quality of your progress notes directly reflects the quality of your clinical work. A comprehensive template ensures that all critical elements of a session—from subjective reports to objective observations and the resulting treatment plan adjustments—are consistently captured. This detailed approach proves that interventions are targeted, evidence-based, and directly addressing the presenting problems outlined in the initial assessment.
Furthermore, effective progress notes are vital for collaborative care. When a client is seeing multiple providers—a psychiatrist, a primary care physician, or other specialists—clear, timely, and thorough notes facilitate seamless communication. A standardized format allows other professionals to quickly grasp the client’s current status, the therapeutic direction, and any recent breakthroughs or setbacks. This article will delve into the essential components of an effective psychology progress note template, explore various structuring methods, and discuss how these documents support both clinical excellence and administrative compliance.
Progress notes are far more than just records of what happened in a session; they are a dynamic reflection of the therapeutic process. They serve multiple crucial functions that underscore their importance in the daily operations of a psychology practice. Understanding these roles helps practitioners appreciate why dedicating time to developing a high-quality template is a worthwhile investment.

From a legal perspective, progress notes act as the primary defense against malpractice claims. They must clearly document informed consent, the rationale for interventions used, and evidence that the client was at risk or made aware of potential risks. Ethically, detailed documentation ensures that the care provided is traceable and aligns with professional standards. If a client’s condition deteriorates, thorough notes detailing previous risk assessments and attempted interventions become invaluable evidence of responsible practice.

A good progress note inherently connects the session to the overarching treatment plan. It answers the question: “What did we do today, and how does it move us closer to our stated goals?” This continuity is essential, especially when a client transitions between therapists or practices. A well-structured note provides a clear narrative arc of the client’s journey, detailing initial symptoms, responses to specific modalities (like CBT techniques or psychodynamic interpretations), and progress metrics. This prevents redundant questioning or shifting therapeutic focus unnecessarily between sessions.

In the contemporary healthcare landscape, documentation is intrinsically tied to reimbursement. Insurance payers require documentation that clearly links the services provided (e.g., 45 minutes of individual psychotherapy) to the client’s diagnosis and the specific necessity of the intervention. A missing or vague note can lead to claim denials or audits. A well-designed Psychology Progress Note Template incorporates fields specifically designed to meet payer requirements, ensuring that the service provided is clearly justifiable based on the documented clinical necessity demonstrated in the note itself.
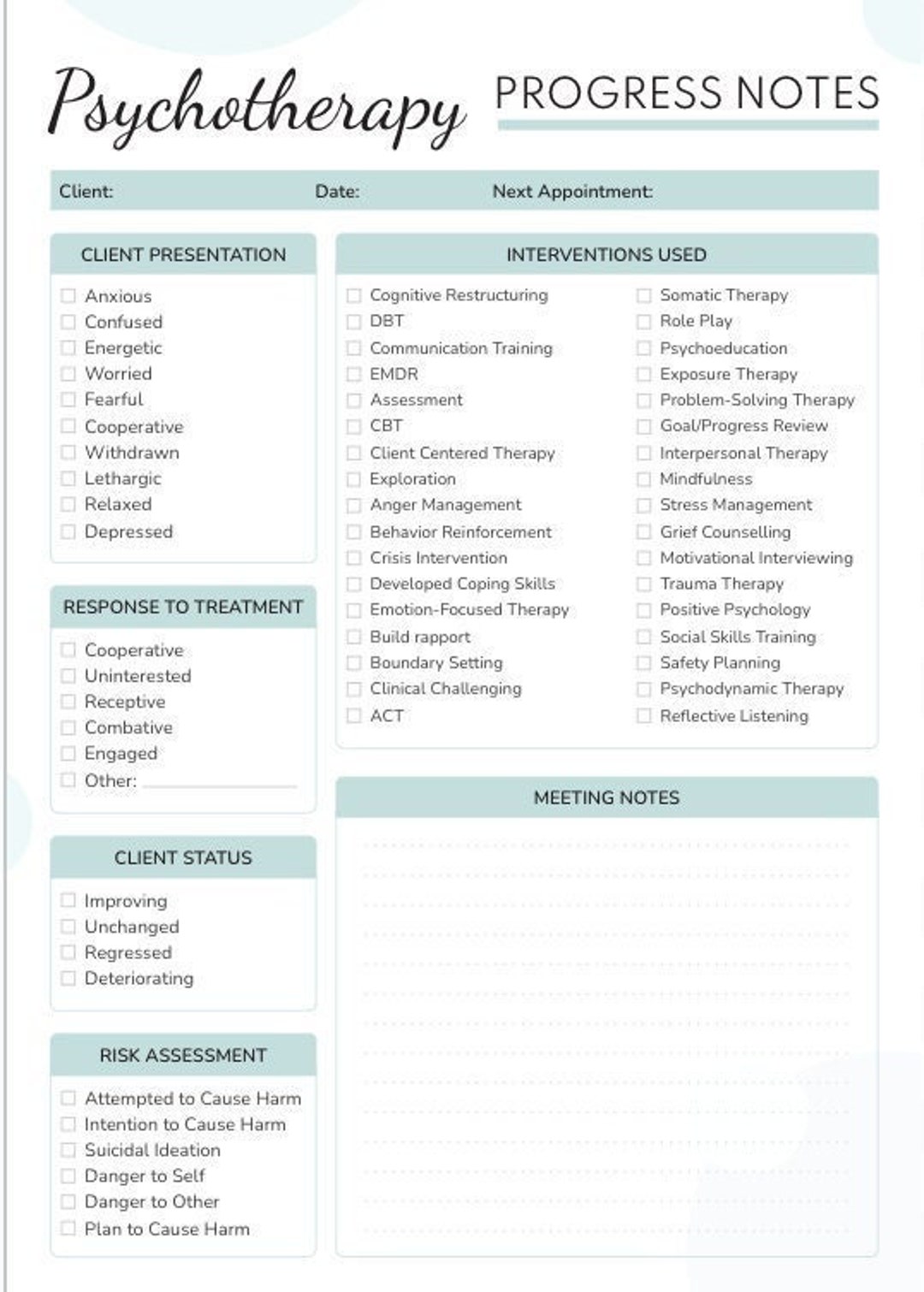
While specific requirements can vary based on setting (e.g., inpatient vs. outpatient, private practice vs. community mental health), a high-quality template must systematically capture key information. The most widely recognized and effective structures often incorporate elements of the SOAP or DAP model, adapted for psychological depth.
The subjective section captures what the client reports. This should be presented in the client’s own words where appropriate, reflecting their current emotional state, reported symptoms, and perspective on treatment progress since the last session.

Key elements to include here are:
* Chief Complaint Update: How the client views their current status.
* Symptom Frequency/Intensity: Quantifiable data on reported anxiety, depression, sleep quality, etc.
* Homework Compliance: Client feedback on tasks assigned in the previous session.
* Reported Feelings/Thoughts: Significant emotional disclosures or cognitive themes from the week.

This section details the clinician’s objective observations regarding the client’s presentation during the session. This should be descriptive and free of interpretation. It relies on observable data.
What to document:
* Appearance and Behavior: Grooming, hygiene, posture, restlessness, or psychomotor agitation/retardation.
* Speech: Rate, volume, and coherence (e.g., pressured, slow, tangential).
* Affect and Mood: Observed range, appropriateness, and stability of affect. Mood should be distinguished from affect (e.g., “Client reports feeling sad [mood], but displayed a flat affect throughout the session [objective observation]”).
* Thought Process and Content: Presence of racing thoughts, suicidal/homicidal ideation (SI/HI), delusions, or obsessions.
The assessment is where the clinician synthesizes the Subjective and Objective data. This section requires significant clinical expertise and forms the core justification for the continued treatment plan.
This segment must address:
* Diagnostic Status: Any changes or confirmations related to DSM-5 diagnoses.
* Clinical Formulation: How the session content relates to the working hypothesis.
* Progress Toward Goals: A concise statement on movement (or lack thereof) toward specific treatment plan objectives.
* Risk Reassessment: A clear statement regarding current risk levels for harm to self or others, based on today’s session.
The plan should outline the interventions used in the session and the plan for the subsequent week or session. This is critical for demonstrating medical necessity.
Elements of the Plan:
* Interventions Provided: Specific techniques utilized (e.g., “Introduced cognitive restructuring worksheet,” “Processed transference related to authority figures”).
* Client Response: How the client engaged with and responded to the interventions.
* Homework/Between Session Tasks: Specific assignments given to the client.
* Follow-Up: Date and time of the next scheduled session.
While the S-O-A-P structure (Subjective, Objective, Assessment, Plan) is ubiquitous across medical documentation, mental health clinicians often find the DAP model (Data, Assessment, Plan) more intuitively suited to therapeutic dialogue. Understanding both allows practitioners to choose or adapt the best Psychology Progress Note Template for their needs.
In the DAP format, the Data section typically combines the Subjective (client report) and Objective (clinician observation) elements into one comprehensive overview of the session’s content.
Many clinicians prefer DAP because it forces a tight integration of observation and report right at the start, leading more directly into the clinical interpretation (Assessment).
Regardless of whether SOAP or DAP is used, modern documentation must be heavily goal-oriented. A robust template forces the clinician to document how the day’s work directly addressed a previously established, measurable treatment objective. For instance, if a goal is “Client will reduce reported panic attacks from four per week to one per week within 60 days,” the progress note must connect the intervention (e.g., diaphragmatic breathing training) to the client’s reported reduction in symptoms. This explicit link is often what auditors search for.
While a general progress note template suffices for routine outpatient therapy, specific clinical contexts demand modifications to ensure comprehensive coverage of unique risks or modalities.
When working with clients who have histories of trauma, the note must reflect sensitivity to potential triggers and the pace of processing. A trauma-informed Psychology Progress Note Template should include sections to specifically document:
CFT notes require documentation of systemic dynamics rather than solely individual pathology. The template must shift focus:
The format in which the template is executed significantly impacts efficiency and data security. Electronic Health Record (EHR) systems provide pre-built, customizable Psychology Progress Note Template options.
Benefits of EHR templates include:
* Time Stamps and Auto-Population: Automatically recording session start/end times, saving manual entry time.
* Security and Compliance: EHRs are designed to meet HIPAA standards for data encryption and access control, minimizing compliance risks associated with unsecured paper files.
* Searchability: Digital notes allow for rapid querying of patterns across months or years of treatment, supporting clinical review and supervision.
To elevate your documentation from merely adequate to exceptionally useful, focus on clarity, conciseness, and clinical justification.
Always assume that someone else—a supervisor, a consulting physician, or a covering therapist in an emergency—will need to read your note. Avoid jargon that isn’t universally understood within your specialty, and write clearly enough that the narrative stands on its own without relying on shared, unspoken context. If you use abbreviations, ensure they are standard or explicitly defined.
A common pitfall is simply listing activities: “Talked about anxiety. Assigned breathing exercise.” This doesn’t demonstrate progress. A better approach integrates the activity with the outcome: “Client participated in 15 minutes of structured relaxation training (breathing exercise), resulting in a reported decrease in subjective anxiety ratings from 7/10 to 4/10 immediately post-intervention.” This shows what you did and what the effect was.
One of the most significant contributors to poor documentation quality is delay. Notes written 48 hours after the session often lack the nuance of immediate recall. Professional standards, and often insurance contracts, mandate completion within 24 to 48 hours. A streamlined Psychology Progress Note Template facilitates this quick turnaround, encouraging documentation immediately following the session while details are fresh.
For practitioners receiving supervision, the note template should have a dedicated space—often within the Assessment or Plan section—to reflect supervisory input and how that guidance was integrated into the current session’s plan. This demonstrates that supervision is actively shaping clinical decisions, which is particularly important for provisionally licensed therapists.
The adoption of a thoughtful and comprehensive Psychology Progress Note Template is indispensable for modern clinical practice. It acts as a multi-functional tool, serving legal protection, communication enhancement, billing justification, and, most importantly, the scaffolding for effective therapeutic delivery. By systematically capturing subjective client reports, objective clinician observations, rigorous clinical assessment, and a targeted plan of action, practitioners can ensure that every session is accounted for, justified, and strategically positioned within the client’s broader treatment trajectory. Investing in a robust, standardized, and regularly reviewed template is an investment in the quality, defensibility, and ultimate success of the therapeutic relationship.