Crafting an effective Procedure Note Template is fundamental to maintaining high standards of patient care, billing accuracy, and legal compliance across all medical specialties. These documentation tools transform complex clinical events into standardized, retrievable records. In the fast-paced environment of healthcare, where every second counts and documentation must withstand rigorous scrutiny, having a robust template ensures that critical details are never omitted, regardless of the provider or the time constraints of the procedure itself. This standardization is not just administrative convenience; it is a cornerstone of quality assurance in medicine.
The necessity for precise procedural documentation extends far beyond simple record-keeping. It directly impacts continuity of care, enabling subsequent providers to understand exactly what was done, why it was done, and how the patient tolerated the intervention. Furthermore, accurate procedure notes are the bedrock for appropriate medical billing and coding, directly influencing revenue cycle management. Without a structured approach, notes can become fragmented, subjective, or incomplete, leading to potential reimbursement denials, increased audit risk, and, most importantly, compromised patient safety due to incomplete historical context.
Mastery over the structure and content of these templates allows healthcare organizations to enforce best practices consistently. Whether dealing with a minor office procedure or a complex surgical intervention, the core components remain essential for comprehensive documentation. Expertise in structuring these templates reflects a commitment to operational excellence and clinical integrity, ensuring that the documentation accurately mirrors the experience and skill applied during the intervention.
This comprehensive guide will explore the critical elements that constitute a best-practice procedure note, delve into best practices for utilization, and discuss how leveraging a standardized Procedure Note Template enhances clinical workflow and legal defensibility. We aim to provide the expertise necessary for healthcare professionals and administrators to implement or refine their documentation standards effectively.
A high-quality procedure note must function as a self-contained document that tells the complete story of the intervention. It should be detailed enough for another expert to understand the sequence of events, yet clear enough for quick review. While the specifics change based on the specialty (e.g., cardiology versus orthopedics), the foundational structure is remarkably consistent.
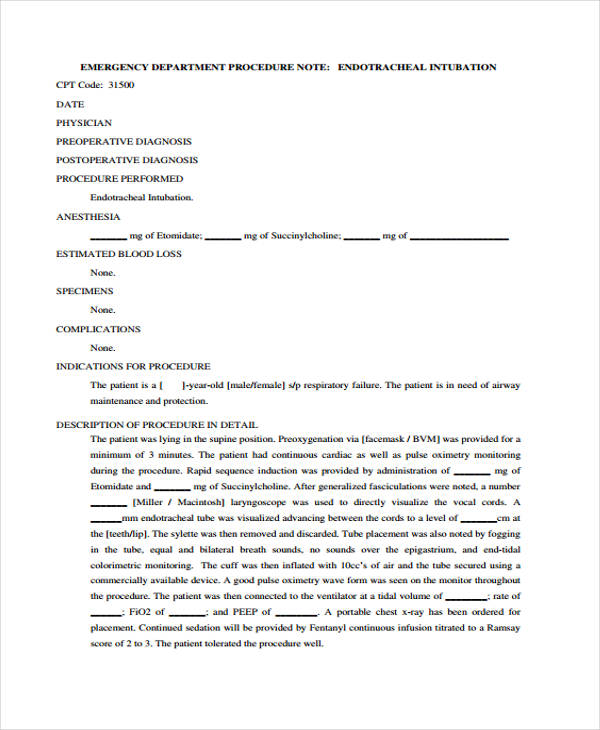
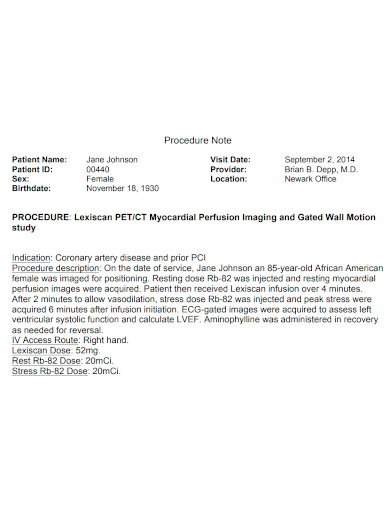
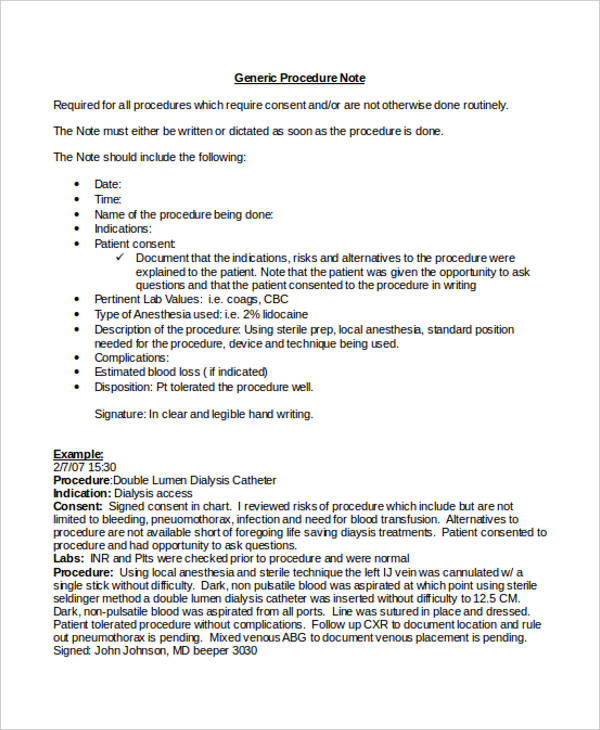
The beginning of any template must firmly establish who and when. This section establishes the legal and chronological context. It must include full patient demographics (name, date of birth, medical record number), the date and precise start/stop times of the procedure, and the names and roles of all personnel involved—the primary surgeon or operator, assistants, and anesthesia provider.
This initial block also demands documentation of the indication for the procedure. This section satisfies the “Why” of the intervention. It must clearly state the diagnosis justifying the procedure and any relevant pre-procedure findings, such as recent imaging results or lab values that informed the decision to proceed.

Trustworthiness in medical documentation is heavily reliant on demonstrating informed consent. The template must dedicate space to confirming that the risks, benefits, and alternatives to the procedure were discussed with the patient or their legal representative, and consent was formally obtained.
Furthermore, the pre-procedure status is vital. This includes documenting the patient’s baseline physical status, relevant allergies, current medications (especially anticoagulants or steroids that might affect the procedure), and confirmation of site marking, which is a critical safety check often mandated by accreditation bodies.
This is the core of the document, requiring the highest degree of expertise. The description should be chronological and methodical, detailing what was done and how it was performed. For surgical procedures, this involves describing the approach, incision sites, dissection planes, specific maneuvers performed, and any significant anatomical findings encountered.
For non-surgical procedures, this area should detail the specific techniques used, the type and amount of local anesthesia administered, and any technical challenges faced. Effective use of the template requires operators to move beyond generic statements. Instead of simply writing “Procedure completed,” a strong note details the manipulation, fixation, irrigation, and closure techniques utilized.
Accurate documentation of findings during the procedure enhances the authority of the note. This section records any unexpected pathologies, anatomical variations, or findings that might influence post-procedure care. If tissue or fluid specimens were collected, this area must meticulously detail:
The documentation must close the loop by describing the immediate post-intervention state. This includes assessing the patient’s immediate tolerance to the procedure, describing the final status of the surgical site or access point (e.g., dressings applied, drain placement, stability of fixation), and any immediate postoperative orders initiated.
Critically, the template must have a dedicated space to explicitly confirm the absence of complications. If any adverse event did occur—even minor issues like unexpected bleeding or delayed response to anesthesia—it must be documented thoroughly, including the intervention taken to manage it and the outcome.
The true value of a Procedure Note Template shines when it moves beyond being a mere checklist and integrates seamlessly into the clinical workflow. Standardization reduces cognitive load, allowing providers to focus their expertise on patient care rather than formatting concerns.
A well-designed template enforces consistency across an entire department or facility. This consistency drastically improves data retrieval for quality audits and research purposes. For example, if every orthopedic surgeon uses the same template to document the insertion of hardware, aggregating data on complication rates related to a specific implant becomes straightforward.
Many electronic health record (EHR) systems offer customizable templates utilizing structured data fields (e.g., drop-down menus for equipment used or specific measurements). This structured data capture is superior to free text for several reasons. It significantly reduces transcription errors, speeds up the completion time, and most importantly for billing, it ensures that all necessary components required for accurate Level 5 coding or surgical package billing are present and correctly formatted.
In the current healthcare landscape, documentation is inextricably linked to reimbursement. Incomplete or ambiguous procedure notes are the leading cause of claim denials. A comprehensive procedure note template acts as a preemptive defense mechanism against coding scrutiny.
The template should prompt the user to document elements directly tied to CPT codes, such as:
By embedding these checks, the template ensures the documentation meets the standards set forth by the Centers for Medicare & Medicaid Services (CMS) and private payers, thereby boosting Authoritativeness and ensuring Trustworthiness in the submitted claims.
Implementing a new template system requires more than just distributing a document; it requires cultural adoption backed by training and continuous refinement. Experience shows that poorly rolled-out templates often face resistance or “template fatigue,” where providers revert to poor habits to save time.
Templates are living documents that must evolve based on real-world Experience. Procedures change, new equipment is introduced, and regulatory requirements shift. A governance structure must be in place to regularly review template performance.
To maximize Expertise utilization, training must focus not just on where to enter information but how to describe procedures accurately. For instance, defining acceptable terminology for dissection planes or suture types ensures uniformity. Ambiguous language such as “cut down to the area” should be replaced with precise anatomical descriptors.
Consistent training reinforces the importance of documentation as a core clinical responsibility, not an administrative afterthought. This focus helps align the team toward a shared standard of excellence.
While the core components remain, the emphasis within the Procedure Note Template must shift depending on the setting. Documentation requirements for a high-risk, operating-room procedure differ markedly from those for an outpatient clinic procedure.
OR notes demand the highest level of detail, especially concerning sterility, equipment counts, and anesthesia management. Here, the template must rigorously document the Time In/Time Out process, confirming counts of sponges, needles, and instruments before closure—a critical patient safety step. The integration of anesthesia flow sheets directly referencing the operative note ensures a comprehensive record of physiological management throughout the intervention.
For procedures performed in an outpatient or office setting—such as biopsies, minor excisions, or joint injections—the focus often shifts slightly towards justifying the visit level and ensuring proper follow-up planning.
In these settings, the template should emphasize:
For procedures reliant on imaging guidance (e.g., angiography, catheter placements, endoscopic procedures), the template must heavily feature the visualization aspect. This includes documenting the specific imaging modality used (fluoroscopy, ultrasound, CT), contrast agents administered (including volumes and reactions), and specific anatomical landmarks visualized to confirm accurate placement or targeting. The level of radiation exposure, if applicable, should also be documented where possible, contributing to overall patient safety records.
In litigation or audits, the procedure note is often the first and most crucial piece of evidence reviewed. A meticulously constructed template provides robust legal protection by demonstrating due diligence and adherence to the standard of care.
Legal defensibility hinges on showing that the actions taken were medically appropriate. This requires clear documentation in the pre-procedure section demonstrating the failure of less invasive management strategies or the urgency of the situation. If a complex procedure was chosen over a simpler one, the Procedure Note Template must contain the dictated rationale derived from the provider’s Expertise.
While a template standardizes input, the system in which it resides must protect that input. Using certified EHR systems that provide audit trails—logging who accessed and modified the note, and when—is paramount for maintaining Trustworthiness. Any changes to a completed note must leave a visible, indelible mark showing the history of revision, preventing accusations of retrospective alteration of events. The template design must align with HIPAA standards for security and access control.
The utilization of a standardized Procedure Note Template is non-negotiable for modern medical practice. It serves as the single source of truth detailing the clinical encounter, bridging the gap between clinical action and administrative necessity. By meticulously incorporating sections covering patient identification, consent, detailed procedural steps, findings, and post-procedure management, healthcare facilities ensure high levels of Experience translation into documented quality.
An expertly designed template drives efficiency, mitigates billing risks, and most importantly, safeguards patient well-being by ensuring that all critical details are recorded consistently. Investing time and Expertise in developing, training staff on, and regularly auditing these templates is a direct investment in operational excellence, clinical Authoritativeness, and unwavering Trustworthiness within the healthcare system. These documents are not just records; they are essential tools for clinical accountability.