The development and diligent use of a standardized Operative Note Template is fundamental to ensuring patient safety, maintaining legal compliance, and optimizing procedural efficiency within any surgical or procedural setting. In the high-stakes environment of healthcare, documentation serves as the definitive record of care, and any ambiguity can lead to significant clinical and administrative complications. These templates act as a critical bridge, connecting the pre-operative planning, the intra-operative actions taken by the surgical team, and the post-operative instructions provided to recovery staff and primary care physicians.
A well-crafted operative note is more than a mere formality; it is a crucial component of the patient’s medical history, often revisited for billing, quality audits, peer review, and—most importantly—to guide subsequent care should complications arise or future procedures be necessary. Inconsistencies in charting can undermine the perceived Expertise and Trustworthiness of the surgical team. Therefore, understanding the essential components and best practices for utilizing these templates is paramount for surgeons, residents, and operating room (OR) personnel alike.
This comprehensive guide will explore the anatomy of an effective operative note, detail the mandatory elements required for compliance, discuss the benefits of digital versus paper templates, and offer insights into how to leverage these documents to enhance overall surgical quality and patient outcomes. Mastery over this documentation process is a hallmark of professional surgical practice.
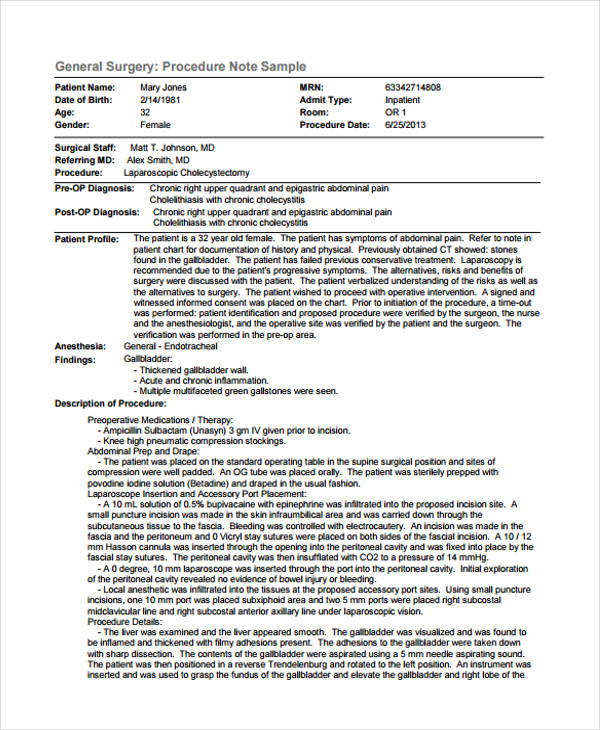
The structure of an operative note must be systematic to ensure that no critical piece of information is overlooked. While specific regulatory requirements might vary slightly by institution or specialty, a core set of elements is universally required to meet standards of care and legal scrutiny.

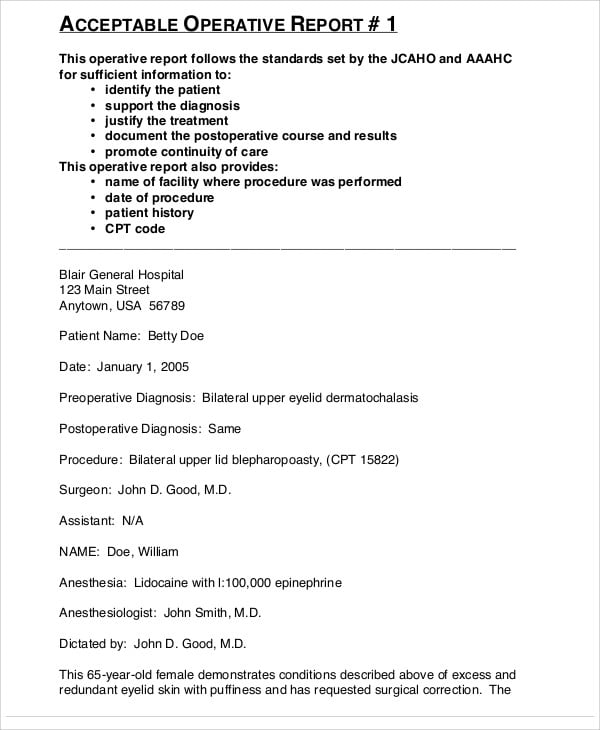
The note must begin by clearly stating the preoperative diagnosis. This establishes the clinical context for the procedure performed. Following this, the postoperative diagnosis must be explicitly documented. Ideally, these two diagnoses should align, but any discrepancies must be explained by findings during the procedure.
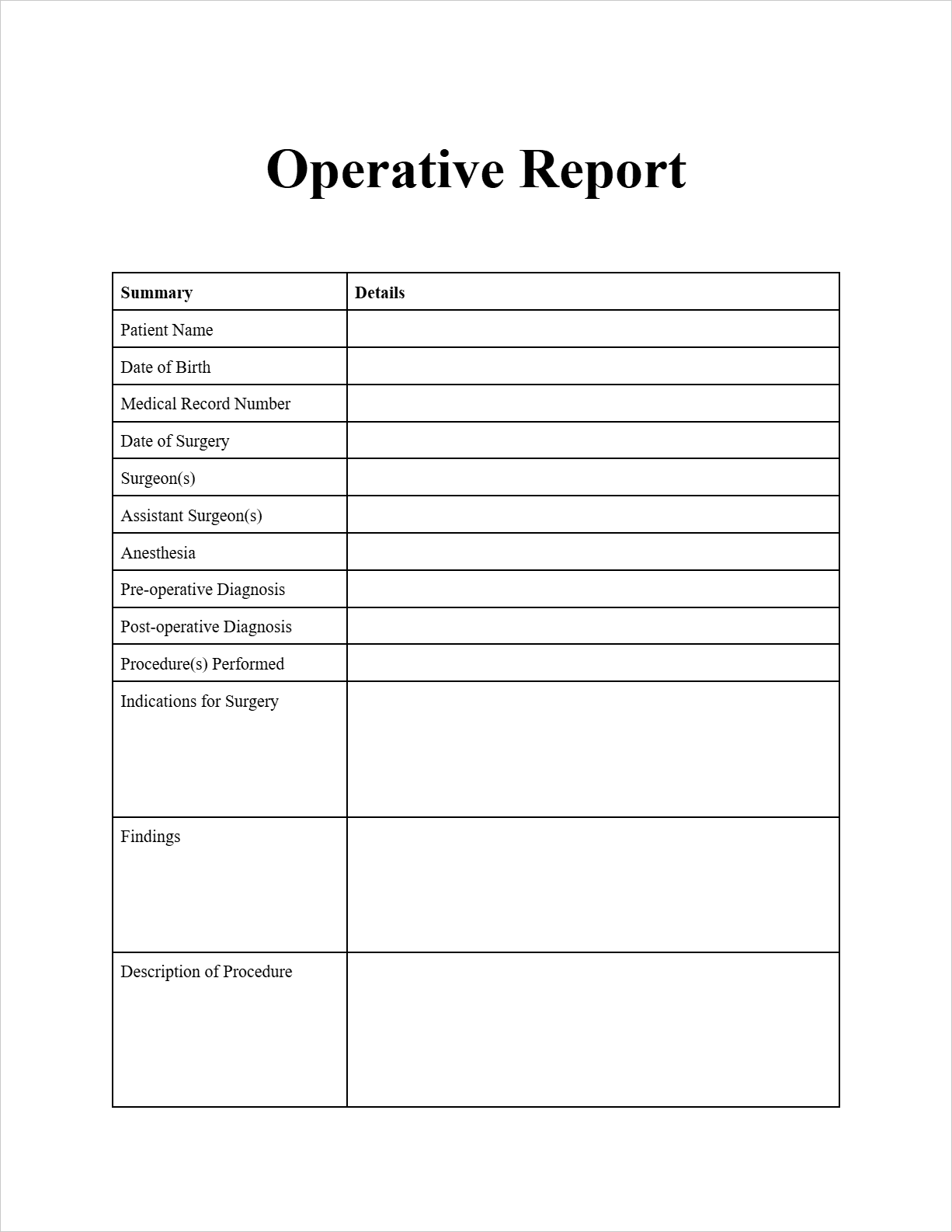
Equally vital is the precise identification of all personnel involved. This includes the primary surgeon, the assistant surgeon(s), the scrub technician, and the circulating nurse. Accurate recording of the primary surgeon’s credentials and the roles of trainees (e.g., residents, fellows) is essential for credentialing and supervision records.

The definitive title of the procedure performed is non-negotiable. If multiple procedures were performed, each must be listed separately. The template must also dedicate space to confirming the informed consent process. This section should confirm the procedure discussed, the risks and benefits explained, and the patient’s acknowledgment, often referencing the signed consent form attached to the chart.
A common area for documentation oversight is ensuring that the procedure performed matches the procedure authorized. This meticulous verification reinforces Authoritativeness and patient safety protocols.

Accurate timing is critical for tracking OR utilization efficiency and for assessing periods of potential patient risk, such as prolonged tourniquet time or excessive anesthetic exposure. The template must clearly capture:
This narrative section is where the surgeon documents the Experience gained during the operation. It must be written in chronological order and describe exactly what was done, not just what was planned. Key elements to detail include:
In the medical-legal landscape, the operative note often serves as the primary piece of evidence regarding the standard of care provided. Failure to document accurately or completely can be interpreted as a failure to meet that standard. Regulatory bodies and insurance payers heavily scrutinize these documents.
The documentation must precisely support the CPT (Current Procedural Terminology) codes submitted for billing. If the operative note fails to describe the complexity or specific steps justifying a higher-level code, reimbursement may be denied. Conversely, over-coding based on vague documentation can lead to audits and fraud allegations. The standardized Operative Note Template helps structure the narrative to include the necessary keywords and complexity indicators required for accurate coding, thus bolstering administrative Trustworthiness.
Accreditation bodies, such as The Joint Commission, require robust quality assurance programs. Operative notes are the raw data source for these reviews. By using a consistent template, auditors can more easily compare outcomes across similar procedures, identify outliers, and pinpoint areas where educational intervention might be needed. This systematic approach strengthens the overall quality framework of the institution.
Modern healthcare largely relies on Electronic Health Records (EHRs), which predominantly utilize digital Operative Note Template systems. These systems offer significant advantages:
However, EHRs also pose risks, such as “note bloat” where excessive boilerplate text obscures the unique details of the specific operation, thereby reducing the clinical utility of the note itself.
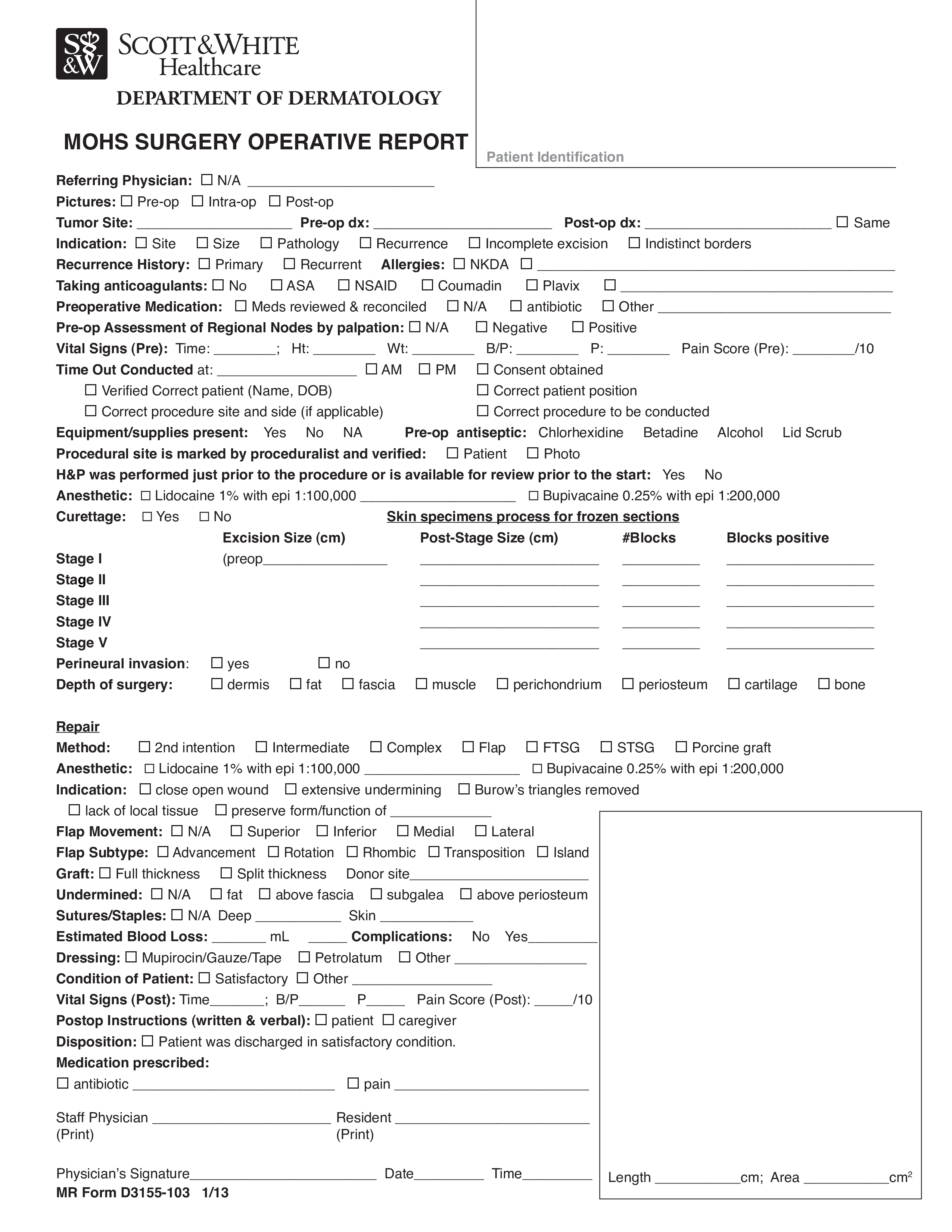
While the foundational structure remains consistent, the level of detail required in the narrative shifts significantly based on the surgical discipline. A general surgery template will differ substantially from one designed for neurosurgery or interventional cardiology.
Orthopedic procedures often require meticulous documentation regarding implants and fixation devices. The template must have dedicated sections for:
Vascular procedures demand extreme precision regarding anastomoses (connections) and graft placement. General surgery templates focus heavily on oncologic margins (if applicable) and the integrity of repairs (e.g., hernia mesh type and fixation). The documentation must clearly articulate the pathology found versus the pre-operative suspicion.
For laparoscopic or robotic procedures, the Operative Note Template must specifically address the entry technique, trocar placement, and any complications related to port placement. Furthermore, the note must confirm that the final specimen removal technique used (e.g., retrieval bag, minilaparotomy extension) was safe and effective. Documenting the use of energy devices and energy settings, while often found in separate logs, should be summarized or referenced.
The successful creation of an operative note is a team effort that begins long before the patient reaches the OR table and concludes immediately after the procedure. Enhancing the team’s Experience with the documentation process streamlines care.
The surgeon should review the template before the case begins. This mental rehearsal ensures that key findings they expect to document are top of mind, leading to more organized intra-operative note-taking, often via dictation or structured electronic input. Residents should be taught to pre-fill non-variable sections like patient demographics and scheduled procedure title.
The ideal scenario involves real-time dictation or structured note-taking during the procedure, though this can sometimes distract from direct patient care. If dictated immediately post-procedure, the surgeon must resist the urge to generalize. The temptation to write “standard closure performed” when specific suture types or tension details matter should be avoided.
For example, when documenting fascia closure, simply stating “fascia closed” is insufficient. A high-quality note confirms Experience by detailing: “Anterior rectus fascia closed using running PDS #1 suture in a simple interrupted pattern with 2 cm bites.”
The final step requires review by the surgeon to ensure completeness and accuracy before the note is finalized and permanently entered into the patient’s record. This review confirms the surgeon’s Authoritativeness over the content. In teaching hospitals, the resident often drafts the note, but the attending surgeon must personally verify every detail before signing, accepting full legal responsibility for the document.
Even with standardized templates, errors persist. Identifying and correcting these pitfalls is essential for maximizing the utility and compliance of the documentation.
The most common deficiency is the over-reliance on boilerplate language copied from previous notes. If a surgeon copies a paragraph describing dissection planes from a prior case where a different approach was needed, the note becomes inaccurate. Search engines and auditors can flag excessive duplication, signaling a lack of genuine engagement with the current case documentation. Maintaining flexibility within the template structure is key.
In procedures involving internal cavity exploration, sponge, needle, and instrument counts are mandatory safety checks. The operative note must explicitly state that counts were correct at the close of the procedure (or document any discrepancy and the resolution process). A missing count section is an immediate red flag for compliance reviewers.
The section detailing immediate postoperative orders (e.g., dressing care, activity restrictions, pain management, anticipated drains management) is crucial for the transition to nursing and recovery care. If these instructions are generic, the risk of post-discharge complications increases. The template must guide the provider to be specific about weight-bearing status or wound care specifics.
As surgical technology advances, so too must the documentation standards supporting it. The trajectory points toward greater integration and automation.
The future Operative Note Template will likely be less of a standalone document and more of a dynamic summary drawn from integrated data sources. This includes automatic population from:
This level of integration leverages technology to enhance the accuracy and efficiency, allowing the surgeon to focus more intently on clinical decision-making rather than transcription, thereby validating the team’s collective Expertise.
There is a growing movement, driven by organizations like the Association for Standardization of Automation and Information Management (AHIMA) and specialty societies, to create benchmark operative note standards. This movement aims to ensure that a note written in one hospital system is easily understood and supports quality benchmarks when reviewed in another, enhancing overall system Trustworthiness.
The Operative Note Template is far more than administrative paperwork; it is the cornerstone of clear communication, legal protection, and continuous quality improvement within surgery. Mastering its structure requires diligence in documenting every step, from the initial pre-operative diagnosis to the final specimen disposition and postoperative orders. By adhering to meticulous documentation standards, leveraging the efficiencies offered by modern EHR templates, and focusing on narrative clarity over boilerplate filler, surgical teams can uphold the highest standards of Expertise, Authoritativeness, and Trustworthiness in patient care. The commitment to a comprehensive and accurate operative record directly translates into safer and better-managed patient journeys.