Effective communication is the backbone of safe and high-quality patient care, making well-designed Nurse Report Sheet Templates indispensable tools in any fast-paced healthcare environment. These templates serve as standardized mechanisms for transferring critical patient information, minimizing the risk of errors, and ensuring continuity of care across shift changes. In the demanding world of nursing, where seconds matter, having a structured, comprehensive reporting tool is not just a convenience—it’s a fundamental safety requirement. The variability in patient acuity, the sheer volume of data generated daily, and the need to adhere to strict regulatory standards necessitate the use of proven, efficient templates that capture every vital detail without becoming cumbersome.
The evolution of nursing documentation has highlighted the critical need for templates that blend traditional clinical insight with modern usability. A poorly structured handoff report can lead to crucial details being overlooked, resulting in adverse patient events. Conversely, a robust template guides the reporting nurse through all necessary checkpoints, from recent vital signs and medication administration to psychosocial assessments and pending physician orders. Mastering the components and application of these essential documentation aids directly impacts patient outcomes and overall unit efficiency.
This comprehensive guide explores the critical elements, best practices, and various formats available for Nurse Report Sheet Templates. We will delve into why standardization is paramount, examine the specific sections necessary for different care settings—such as ICU versus med-surg—and discuss how these tools contribute significantly to reducing medical errors. By understanding the engineering behind an effective report sheet, nurses can transform the often-stressful shift change into a streamlined, professional exchange of life-saving data.
Standardization in patient reporting is not merely bureaucratic overhead; it is a direct function of patient safety initiatives championed by organizations like The Joint Commission. When every nurse uses the same format, the brain of the receiving nurse is primed to look for specific pieces of information in a predictable order. This predictability is vital during the high-stress transfer of care.

Inconsistent reporting is a significant vector for medical errors. When a nurse relies on free-form notes or memory cues, the risk of omitting critical data points—like a new allergy, an impending critical lab result, or a subtle change in neurological status—skyrockets. Structured Nurse Report Sheet Templates mitigate this by forcing the reporter to address every required category systematically. This adherence to a checklist or structured format ensures comprehensive data capture.
For instance, if a template mandates a section specifically for “Critical Values Pending/Received in Last 4 Hours,” it ensures that even if the verbal report is rushed, the written artifact contains the necessary context for follow-up, thereby bolstering Trustworthiness in the documentation process.
As subject matter experts in clinical documentation, we recognize that the best templates reflect deep nursing Experience and Expertise. They are not simply blank pads; they are curated instruments designed around evidence-based practices. Effective templates often incorporate elements derived from validated communication tools, such as the I-SBAR-R (Identify, Situation, Background, Assessment, Recommendation, Read back) framework, embedded directly into the physical layout of the sheet.
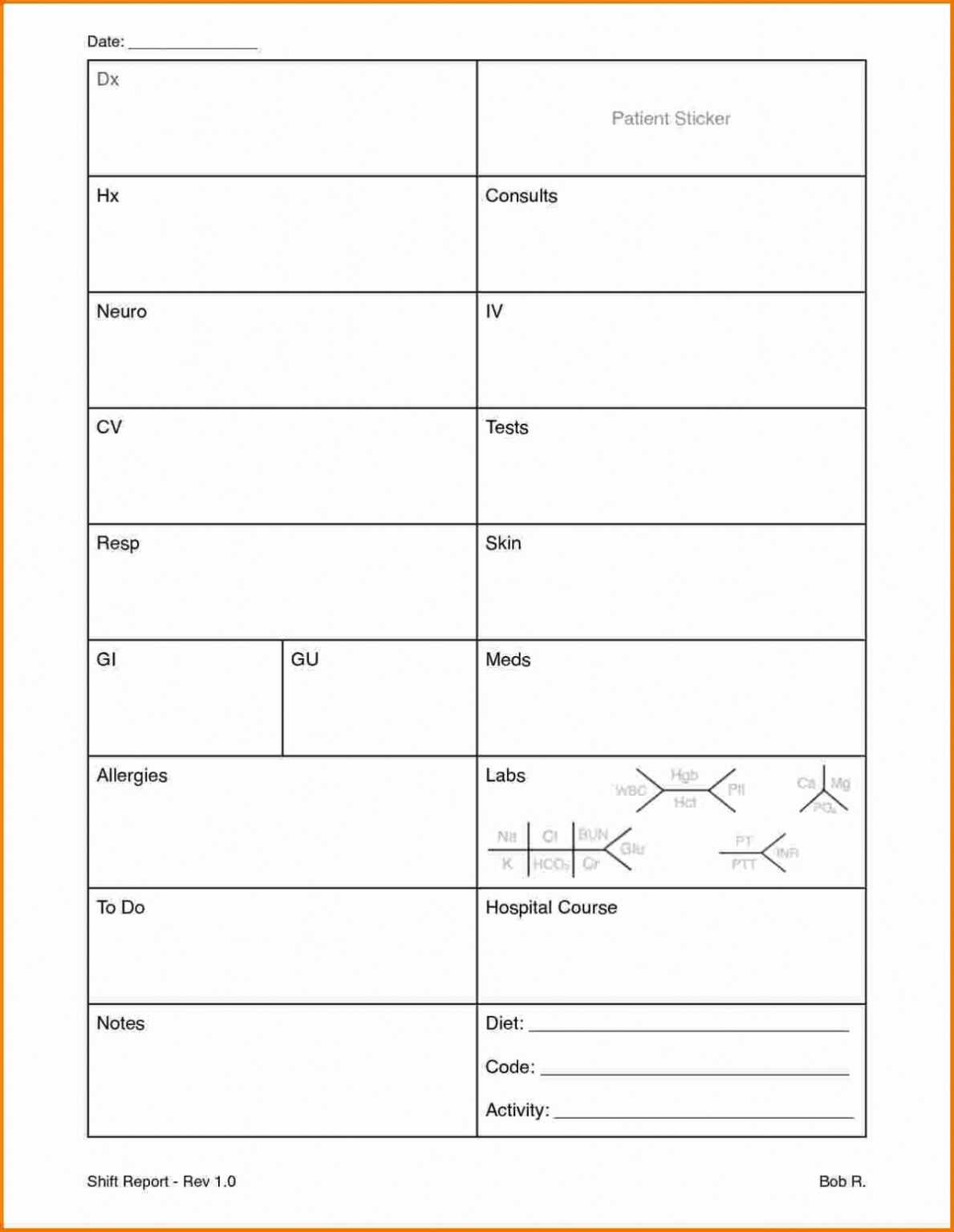
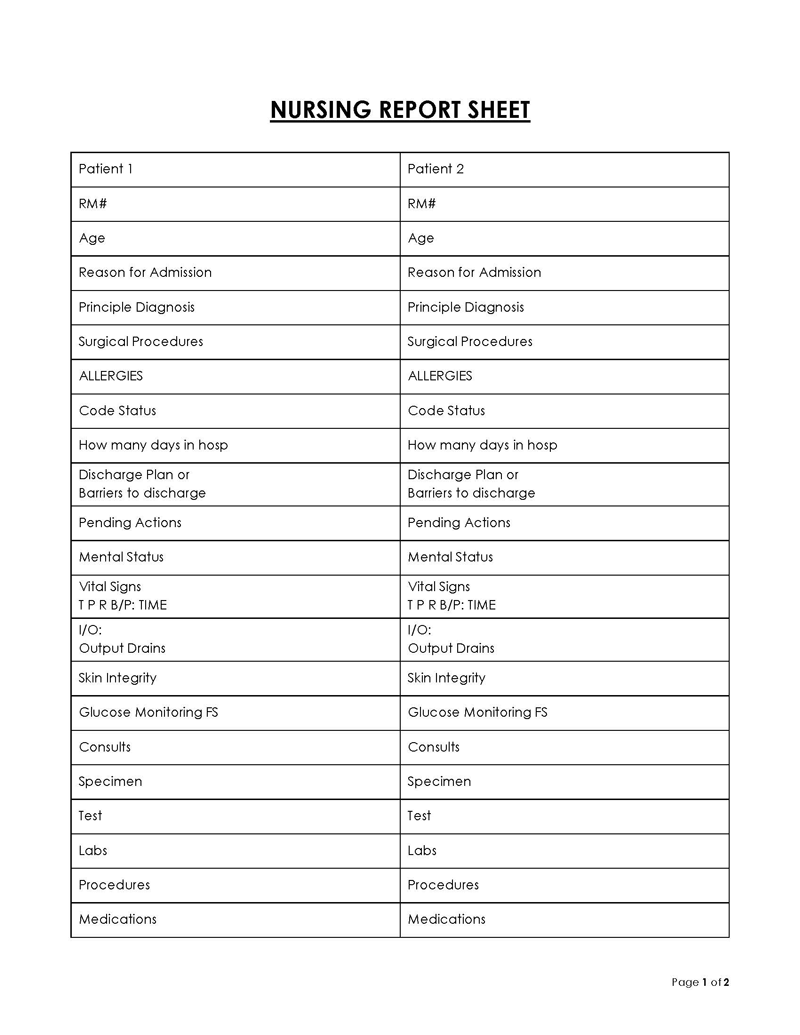
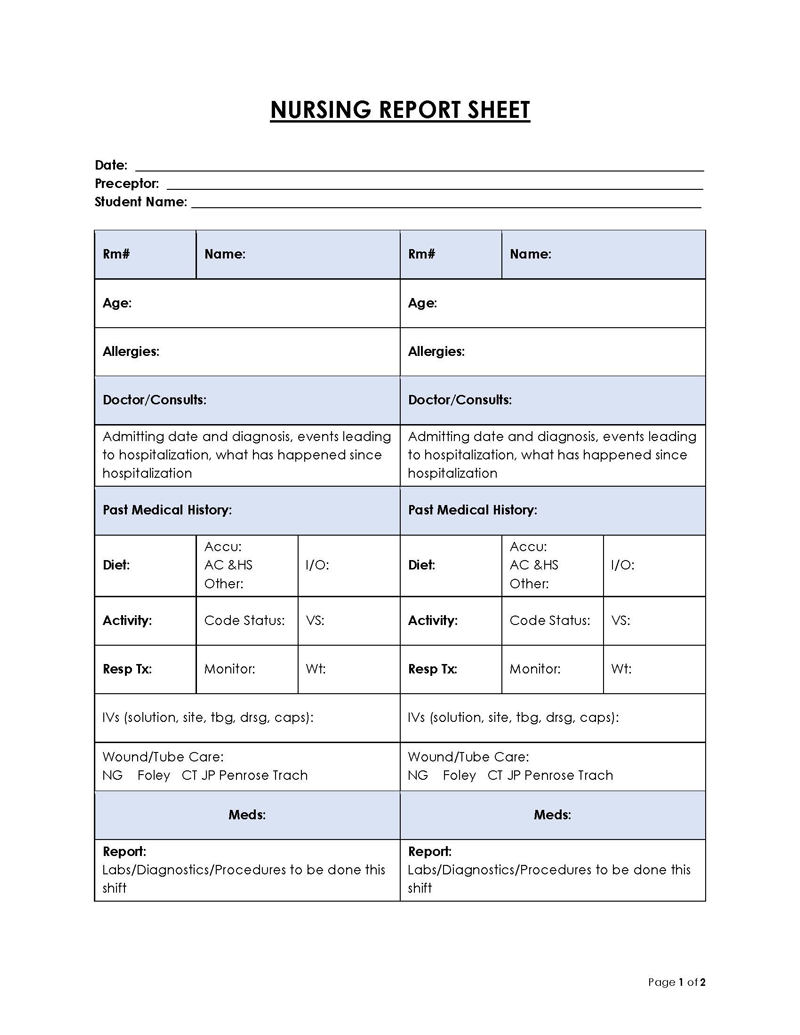
A truly effective template must balance detail with brevity, ensuring all pertinent information is captured without creating an unmanageable volume of paperwork. The optimal structure varies slightly between acute care settings, but core components remain universal across reliable Nurse Report Sheet Templates.
This foundational section ensures proper patient identification and immediate situational awareness.
This is where the quantifiable, recent data points that drive immediate clinical decisions reside.
This section addresses the patient’s experience and the planned interventions for the upcoming shift.
The utility of a template is directly tied to its context. A generalized template may fall short in highly specialized areas. Therefore, developing specialized Nurse Report Sheet Templates for different units demonstrates a higher level of clinical Authority.
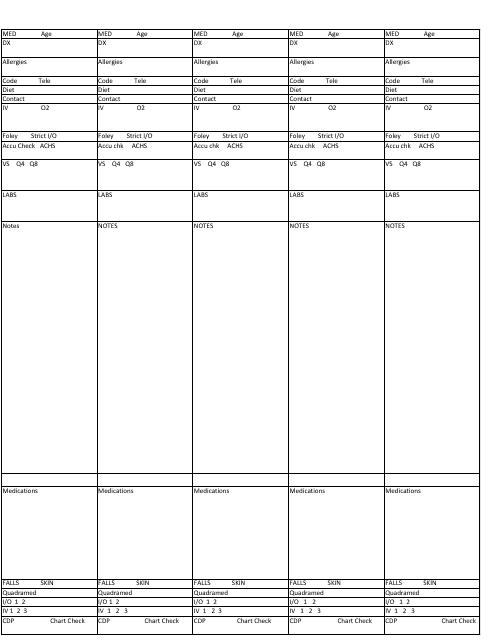
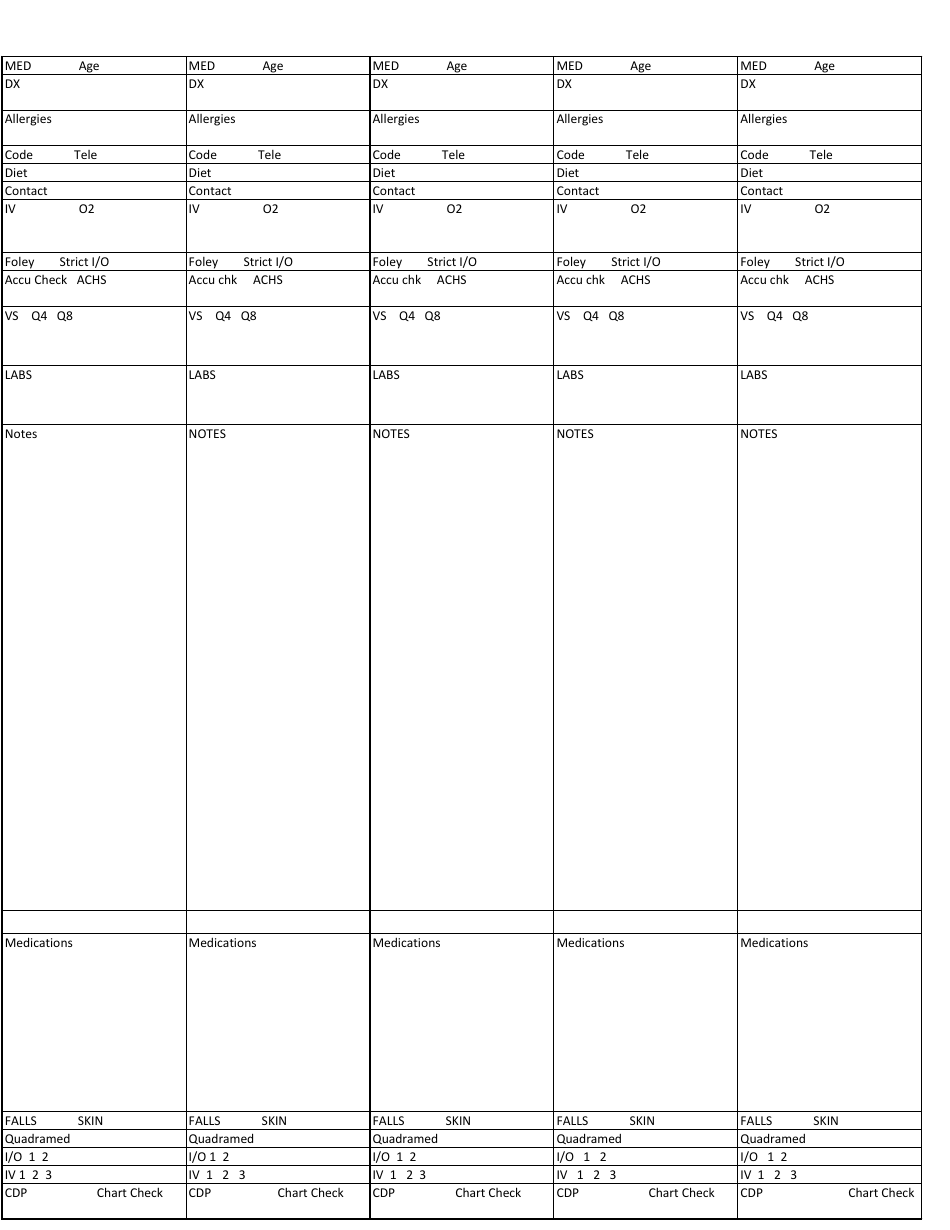
Med-surg templates are often the most generalized, balancing acute care needs with general patient maintenance. They must accommodate patients with diverse pathologies. A key feature here is the clear tracking of mobility status and fall risk protocols, often integrated with a visual scale or flag system directly on the sheet. The structure needs to accommodate a higher volume of routine medications and assessments compared to critical care.
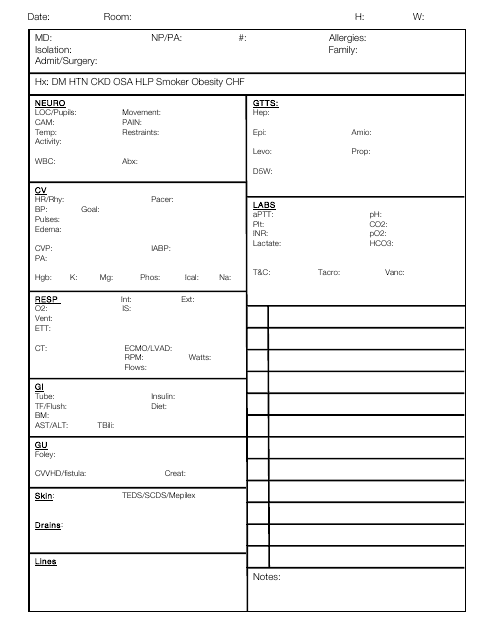
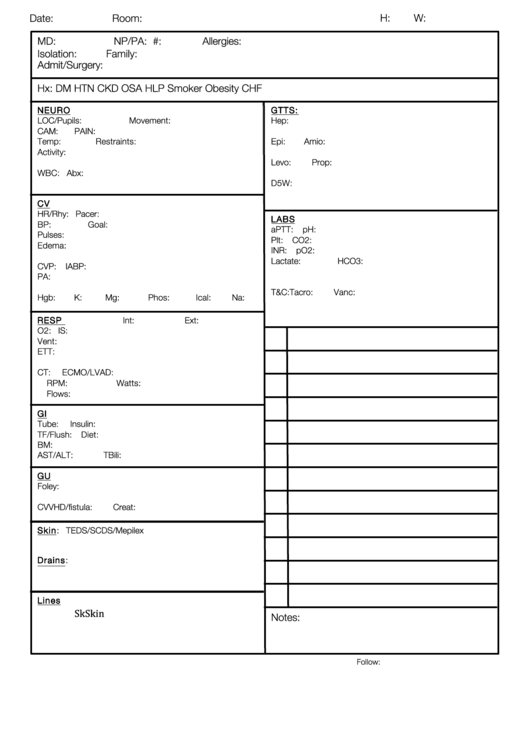
ICU templates require extreme granularity, often focusing on hemodynamic stability and complex interventions. These sheets often look more like a mini flow sheet integrated with narrative reporting sections. They must explicitly track:
The complexity here demands highly structured data entry to maintain the high level of surveillance required for critically ill patients.
In the post-anesthesia care unit (PACU), speed and clarity regarding anesthetic agents and immediate surgical outcomes are paramount. These templates emphasize:
Owning the right template is only half the battle; maximizing its effectiveness requires established best practices for both the reporting and receiving nurse. These practices build Trust in the system itself.
While the template provides the structure, the verbal report allows for nuanced conversation, clarification, and emphasis. The written template should serve as the anchor for the verbal report, not a script to be read verbatim.
The reporting nurse should use the template to guide the narrative, pointing to critical sections (e.g., “As you can see in the Critical Labs box, Mrs. Smith’s potassium spiked overnight…”). This dual approach ensures that context is provided for the static data.
Time constraints are the primary enemy of thorough reporting. Nurses must develop the Experience to pre-populate the report sheet throughout their shift, rather than attempting to compile everything in the last few minutes. Key documentation points—like the administration of a critical antibiotic or a significant patient complaint—should be immediately logged onto the report sheet template as they occur.
Furthermore, utilizing abbreviations consistently and clearly defined within the unit policy prevents ambiguity and speeds up the writing process.
For quality improvement purposes, many facilities audit their shift handoffs. A well-populated Nurse Report Sheet Template serves as tangible evidence of due diligence. Auditing should focus on whether all mandated fields were completed and if the data accurately reflects the patient’s status at the time of transfer. This feedback loop is essential for continually refining the templates themselves based on real-world operational challenges.
The healthcare industry is rapidly moving toward electronic health records (EHRs), yet many facilities, especially those focused on rapid response or those with legacy systems, still rely on paper-based or print-and-fill templates. Understanding the advantages and disadvantages of each is crucial for effective implementation.
Paper templates offer simplicity and immediacy. They do not suffer from login errors, system downtime, or battery depletion. In situations where technology fails, a well-designed paper template ensures continuity of care is preserved. Many veteran nurses prefer the tactile experience, arguing that reviewing a physical summary allows them to focus solely on the patient without digital distractions. The Expertise of older nurses often shines when they can annotate a physical document freely.
Modern EHRs increasingly incorporate standardized handoff tools, which are essentially digitized, often mandatory, Nurse Report Sheet Templates. These digital formats offer several high-value features:
However, digital systems can sometimes be cumbersome, requiring excessive clicking or navigating through multiple tabs, which can slow down the verbal exchange if not optimized for a rapid handoff scenario.
While purchasing pre-made templates or relying on EHR defaults is common, adapting or designing custom sheets based on unit-specific needs can significantly enhance efficiency. This requires a deep dive into the unit’s most frequent critical events and data needs.
The first step in design must address the core patient population. Does your unit primarily manage complex discharges (requiring strong discharge planning sections) or rapid cycling of trauma patients (requiring hemodynamic stability checklists)? Use your existing quality data to identify the top three areas where errors or omissions have previously occurred—these areas need the most prominent space on the new template.
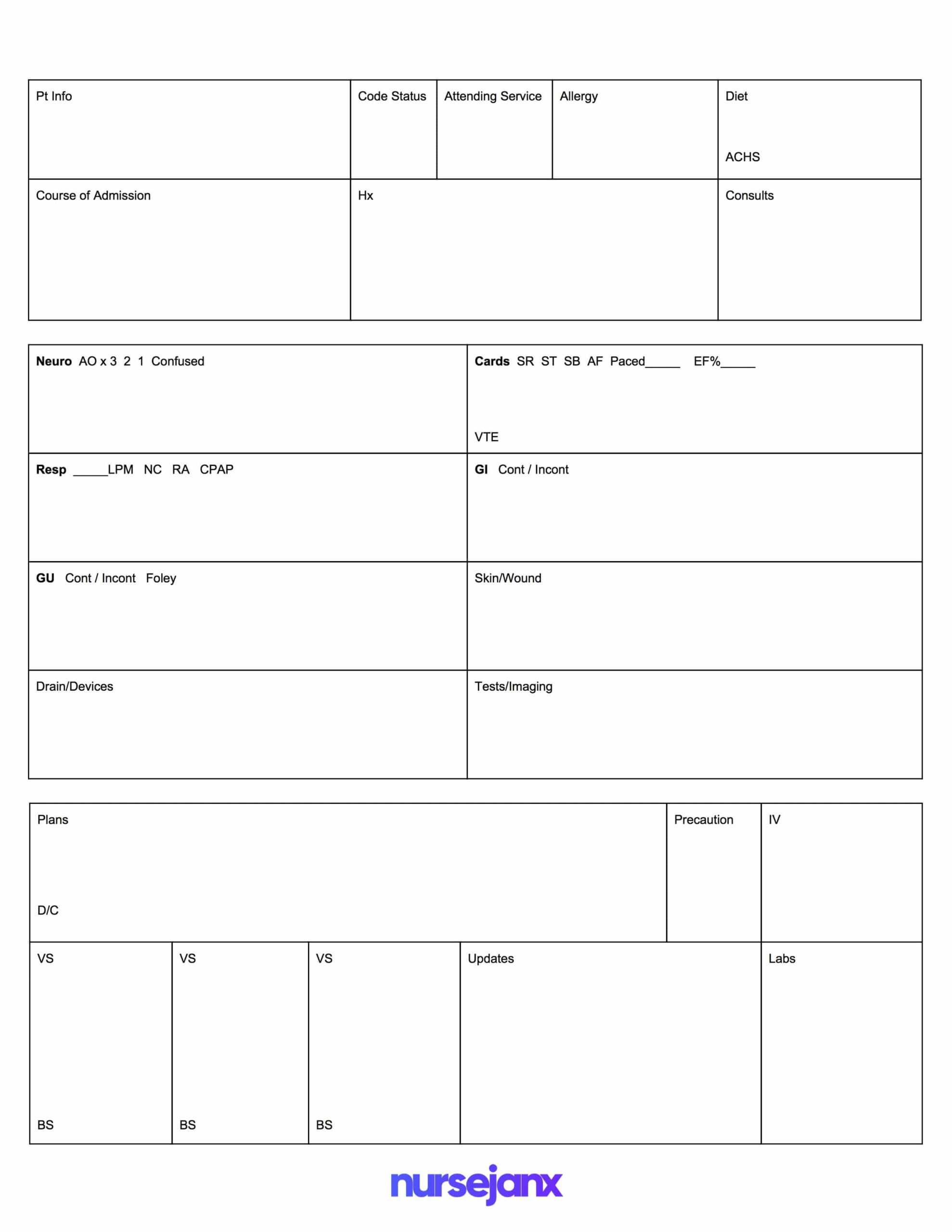
Use visual cues—layout, spacing, and simple iconography—to prioritize information. The most critical, immediately actionable data (e.g., unstable vitals, pending STAT orders) should occupy the top third of the page. Less urgent but necessary ongoing care items can occupy the bottom. This hierarchical structure leverages cognitive psychology to ensure the receiving nurse sees the “need to know now” information first, a testament to applied clinical Experience.
A successful template is dynamic. After implementing a new version of your Nurse Report Sheet Templates, schedule a mandatory review session with nurses from all shifts (day, evening, night) after a set period (e.g., two weeks). Ask pointed questions: “What information was missing?” “What took too long to find?” Use this direct feedback to iterate and improve the documentation tool, continually strengthening its Trustworthiness and utility.
The selection, design, and diligent use of Nurse Report Sheet Templates are fundamental elements of modern, high-reliability healthcare delivery. These standardized tools transcend mere paperwork; they are critical safety interventions that bridge the gap between shifts, ensuring that the nuanced, complex narrative of a patient’s status is transferred accurately and efficiently. By rigorously adhering to structured reporting, incorporating unit-specific data requirements, and actively seeking feedback for continuous improvement, healthcare teams can harness these essential templates to reduce errors, improve team communication, and, most importantly, safeguard the well-being of every patient under their care. Mastery of these documentation practices underscores true nursing professionalism and expertise in complex clinical environments.